Head banging, thumb sucking and toe walking concern many parents
Are head banging, thumb sucking and toe walking serious issues? An article in American Family Physician describes the following:
A young boy, 2½ years of age.… From the time the child was 12 months old, every night, he sat up in bed and repetitively banged his forehead against the wooden crib bars from 1 to 2 hours, after which the child went back to sleep.… Daytime behavior was described as normal.1
Head banging has been reported in 3.3 to 15.2 percent of “normal” children.2 But it is more common in children with cerebral palsy, mental retardation, schizophrenia, autism, otitis media, teething, decreased visual acuity and certain genetic syndromes.3
The medical approach to head banging, thumb sucking and toe walking
I’ve often said that some of the most ridiculous things are found in medical journals. Head banging is serious yet the medical profession considers head banging a relatively harmless way of releasing tension. “If the sound of your baby’s head banging bothers you, try moving the crib away from the wall. Also, be sure to tighten the screws and bolts on his crib regularly.”4 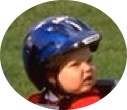 A helmet is sometimes recommended.5
A helmet is sometimes recommended.5
What causes head banging? Medically the cause is unknown. The psychoanalytic school believes head banging is a manifestation of poor ego identity6 and even maternal deprivation.7 The latter appears related to the discredited “refrigerator mother” school of autism etiology.
 However, head banging, head rolling, thumb sucking and other repetitive behaviors may be indicative of cranial subluxations either causing or resulting from meningeal stress. These subluxations/meningeal stresses are often the result of neurological damage caused by pre-natal or birth trauma, accidents, vaccinations, chemical stress and/or emotional stress. Anger and other extreme emotions tighten the meningeal system and increase brain pressure; consequently, head banging is sometimes associated with tantrums.8
However, head banging, head rolling, thumb sucking and other repetitive behaviors may be indicative of cranial subluxations either causing or resulting from meningeal stress. These subluxations/meningeal stresses are often the result of neurological damage caused by pre-natal or birth trauma, accidents, vaccinations, chemical stress and/or emotional stress. Anger and other extreme emotions tighten the meningeal system and increase brain pressure; consequently, head banging is sometimes associated with tantrums.8
Repetitive rocking appears to be an attempt to release pressure on the brain and nervous system.9-12
Accommodation to pressure
Cranial movement appears to help the body adapt to changes in air pressure. If the bones of the skull are subluxated, proper accommodation cannot occur and meningeal stress on the brain and nervous system cause pain and discomfort. That’s why children become hypersensitive when a storm is on the way.
According to an osteopathic source, “Head banging is often an indicator of stresses within the head, and not simply a sign of frustration.”13
Congressional testimony
In Congressional testimony, John E. Upledger, DO, developer of CranioSacralTM Therapy, reported:
Many autistic children are known to bang their heads, chew on their wrists and/or the bases of their thumbs until deep tissue (tendon sheath) is visible, and/or they may suck on their thumbs so vigorously that the front upper teeth begin to displace forward.
Actually, these thumb-sucking children are pressing on the roof of the mouth as hard as they can. We have observed that, when specific corrections of the craniosacral system are successfully carried out, these behaviors spontaneously cease.
It is my opinion that the head-banging child is trying to release a compressive force in the head that is quite painful. When we release this compression, head banging stops.14
 It may be no coincidence that head banging in some children occurs when walking begins since, at that stage, the lower back or lordotic curve forms which adds length to the spinal cord and may increase meningeal tension.15
It may be no coincidence that head banging in some children occurs when walking begins since, at that stage, the lower back or lordotic curve forms which adds length to the spinal cord and may increase meningeal tension.15
What needs to be done for head banging, thumb sucking and toe walking?
Head bangers appear to be trying to relieve cranial/meningeal stress or pain. When meningeal and structural stresses are relieved head bangers have often responded favorably.
Alex was given [cranial] osteopathic treatment after the second treatment his chronic head banging stopped.16
A 3½-year-old autistic female compulsive head banger had a “50% reduction in head banging” under chiropractic care.17
However, cranial work was not included in this child’s care. Had this child additionally received cranial care the reduction would have no doubt been 100%.
In over twenty years of practice with thousands of brain-injured children we have found brain tension due to severe cranial sacral pressure due to the temporal bones and sphenoid basilar junction being “stuck” in addition to intense myofascial strain. After Koren Specific Technique (KST) was added to our protocol we have seen even more rapid progress in creating good cranial rhythm, reducing fascia strain and eliminating head banging. Matt Newell, Director of Family Hope Center, Norristown, PA18
Toe walking
 In addition to head banging and thumb sucking it has been observed that toe walking, another symptom of meningeal tension, can be relieved with proper care. In a personal communication to the author Kevin Johanson, DC of Beaumont, Alberta, Canada writes:
In addition to head banging and thumb sucking it has been observed that toe walking, another symptom of meningeal tension, can be relieved with proper care. In a personal communication to the author Kevin Johanson, DC of Beaumont, Alberta, Canada writes:
A three-year-old was brought in for care because he was a toe walker. After one visit using KST procedures, he stopped walking on his toes.
What to check for
All cranial bones may subluxate; however, using Koren Specific Technique (KST) analysis procedures, we have found the following subluxations most common:
- Sphenoid (left and right wings)
- Occipital bone
- Temporal bones
- Frontal bone
When the sphenoids and occiput are subluxated the proper function of the sphenobasilar junction that pumps cerebrospinal fluid (CSF) may be impaired.
 Please keep in mind that every skull is different. Birth trauma may subluxate a part of the skull that is not anatomically “supposed” to be subluxated. That is especially true if there are bumps, ridges, indentations and other unusual landmarks on the child’s skull.
Please keep in mind that every skull is different. Birth trauma may subluxate a part of the skull that is not anatomically “supposed” to be subluxated. That is especially true if there are bumps, ridges, indentations and other unusual landmarks on the child’s skull.
Of course, the upper cervical spine should be checked for subluxations. We find the following cervical subluxations most common:
- Atlas C1 right posterior arch posterior/lateral (Blair listing)
- C7 usually inferior (spinous listing)
Correcting cranials using KST
 Koren Specific Technique easily and quickly analyzes and corrects or adjusts the entire structural system, including the cranial bones with low force, in the order the body wishes the structures corrected. In addition to being able to locate and correct subluxations to a high degree of specificity on patients, KST practitioners can also specifically analyze and correct themselves!
Koren Specific Technique easily and quickly analyzes and corrects or adjusts the entire structural system, including the cranial bones with low force, in the order the body wishes the structures corrected. In addition to being able to locate and correct subluxations to a high degree of specificity on patients, KST practitioners can also specifically analyze and correct themselves!
References - Click to view
2. Delissovoy V. Head banging in early childhood: a study of incidence. J Pediatr. 1961;58:803-805.
3. Hyman SL, Fisher W, Mercugliano M, Cataldo MF. Children with self-injurious behavior. Pediatrics. 1990;85(3 Pt 2):437-441.
4. http://www.babycenter.com/refcap/baby/babysleep/7556.html by the Baby Center editorial staff.
5. Dawson-Butterworth K. Head banging in young children. Practitioners. 1979;222:676-679.
6. Baumeister AA. Origins and control of stereotyped movements. Monogr Am Associ Ment Defic. 1978;3:353-384.
7. Brody S. Self-rocking in infancy. J Am Psychoanal Assoc. 1960;8:464-491.
8. Berkson G. Early development of stereotyped and self-injurious behaviors: II. Age trends. Am J on Mental Retardation. 2002;107(6):468-477.
9. Retzlaff EW et al. Nerve fibers and endings in cranial sutures research report. J Amer Osteopathic Assn. 1978;77:474-475.
10. Retzlaff E, Mitchell F, Upledger J, Biggert T. Aging of cranial sutures. Anat Rec. 1978;190:520.
11. Retzlaff E, Mitchell F, Upledger J, Biggert T, Vredevoogd J. Temporalis muscle action in parietotemporal suture compression. Presented at 22nd Annual Research Convention of American Osteopathic Association, Chicago, 1978.
12. Retzlaff EW, Michael D, Roppel R, Mitchell F. The structures of cranial bone sutures. J Amer Osteopathic Assn. 1976;75(6):607-608.
13. Sutherland Cranial College http://www.scc-osteopathy.co.uk/learning.php
14. Testimony of John Upledger, April 6, 2000. Gov’t Reform Committee of the U.S. House of Representatives, 106th Congress (1999-2000). http://www.upledger.com/Clinic/autism.htm
15. Silberstein RM, Blackman S, Mandell W. Autoerotic head banging: a reflection on the opportunism of infants. J Am Acad Child Psychiatry. 1966;5(2):235-242.
16. Centers S. Autism. http://www.osteopathiccenter.org/autism.html
17. Warner SP, Warner TM. Case report: autism and chronic otitis media. Today’s Chiropractic. May/June 1999.
18. Matt Newell, Director of Family Hope Center, Norristown, PA. Personal correspondence to author, February 6, 2006.
Learn Koren Specific Technique (KST) through a home study program and at a live seminar. For more information on home study and live seminars go to www.korenspecifictechnique.com or call 267-498-0071.
Please scroll down below to leave me a comment.
And please share this far and wide – patients, colleagues, friends & family!
The buttons are on the right.=====>


Dr. Tedd Koren
Dr. Koren, originally from Brooklyn, NY, lives in Montgomery County, PA. A graduate of the U of Miami and Sherman College of Chiropractic, he writes, lectures and teaches in the US, Europe and Australia as well as takes care of patients and fights for healthcare freedom. Dr. Koren and his wife Beth have two children.




{kind=link}
Excellent Articles.
Thank You Very Much.
Dr Hoang DC,PhD, MD
Thank you Dr Koren, very nice to now understand the relationship between these problems and the cranial bones and the meningeal fixations. I’ll keep this article in my book of references for those cases in the future times.